













A little while back, I started looking around to make a kit of stim tools that I could use to help me sit through long meetings and lectures. Although the combination I’ve settled on (for now) isn’t perfect, I thought it might be helpful to share what I’ve learned and what I’m doing right now.
It’s widely known that autistic people make use of stim tools like the ones I’m going to be talking about. For autistic people, using stim tools may be a method of stimming or “repetitive behaviors”. Many ADHDers use stim tools as well. However, it’s not just autistics and ADHDers who can benefit; for example, bipolar people can definitely use them, particularly in a manic (or mixed) phase. Stim tools can also be used by people who struggle with compulsive behaviors like skin picking (dermatillomania) or hair pulling (trichotillomania). Finally, stim tools can be used to help anyone, regardless of diagnosis!
I started out making a single stim kit, but I soon found it might be more beneficial to make several kits of different sizes. However, the first “stim kit” I want to talk about doesn’t usually come out of a box or a bag — I’m talking about wearable stim tools! Chewable necklaces are very popular among people who bite their nails or non-chewable objects such as pencils. Mine, though, is a little different…
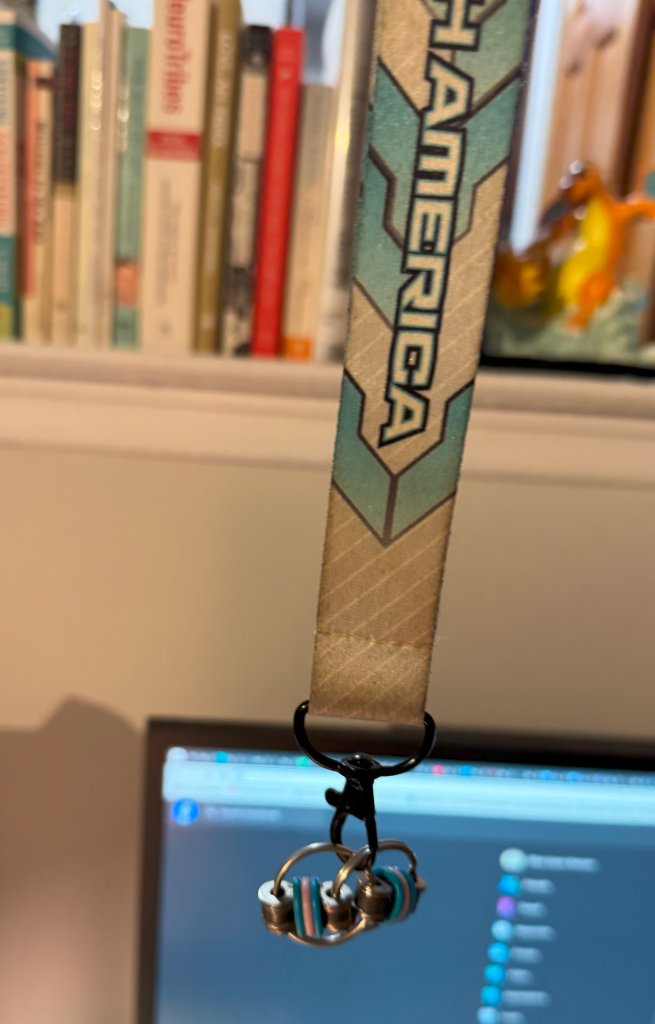
I made this out of a lanyard (this one is from the Pokémon North American International Championships a few years ago) and a bike chain keyring fidget. This is often my go-to stim tool as I wear it around my neck and don’t have to fumble around in my bag for it. It’s also pretty cheap; there are multiple Etsy listings for $5 plus shipping (like this one) and even listings for fun pride-themed colorways which I might just buy right now! Be right back! (By the way, I have no affiliation with any of the products I may link to in this article, nor am I receiving any compensation for including them.) Anyway, these little fidgets are silent, small, and I think they make a particularly satisfying stim for people who may be prone to skin picking. And you can use any lanyard your heart desires!
Now, onto the actual stim kits…

I’ll call the smallest one the “pocket kit” because it just fits in the front pockets of my jeans (American Eagle Womens’ Jeggings). It easily fits in the front pocket of my mini backpack, as well as my bigger backpacks. As you can see, I’m using a Pokémon box (this will be a theme) which is on sale at the Pokémon Center for $20. It also comes with dice and cute status markers for playing Pokémon Trading Card Game, but my favorite asset was this box. So what’s in it?

I’m looking for new stim tools that will fit in the pocket kit, so if you have any recommendations, please send them to me! I really want to hear from you.
Next, the medium kit…

This one is also related to Pokémon! It’s a Japanese deck box. One of my favorites, so it seems fitting I put some stim tools in there. If you’re not familiar with deck boxes, they are generally not too large. I think this one is around 3 in (height) x 3 in (depth) x 4 in (width). The NeeDoh Nice Cube just fits inside.

That’s right… everything in the medium kit is a cube! (✿◡‿◡) A happy little accident.

Now, I don’t want to lie to you, so here it is: a fidget spinner can just barely fit in the deck box I’m using for the medium kit. But, I’m afraid of doing damage to the box by overloading it… so my 2 fidget spinners were included in this amazing bag I got from the Pokémon Center. It’s sparkly! But any toiletry bag should do. Pick your favorite or buy one that suits you!

Have I missed an important stim? Let me know in the comments!
There are some stim tools that can’t be carried around in a box or a bag, but rather, are meant to be used at home or in a private space. Here are some of those things:
So that’s what I’ve learned! Share in the comments your favorite stim tools and how they help you!
Elliot Gavin Keenan arrives as a first-year PhD student in psychology at UCLA. He is autistic and bipolar, aspects of himself he has learned to work with; however, under the sunny Los Angeles sky, something changes. Manias become darker, more distressing, and the cycle of mania and depression accelerates until the boundaries of each state are indistinguishable. By April, Elliot decides to commit suicide. He wakes up in an ICU three days later.
Luminous Mind is about one young trans man’s struggle with mental illness and the paradoxical trauma experienced by suicide attempt survivors. His rhapsodic prose captures hope, despair, ambivalence, and everything in between. Deeply introspective and honest, Luminous Mind is a story of healing.
Do you know anyone with bipolar disorder? This book might just give you the insight to understand that person a little better. Or, if you have bipolar, maybe you’ll learn something about yourself!
Have you ever attempted suicide? Luminous Mind explores healing after experiencing things few people can relate to.
Do you like poetry? There are several original poems in the book! In addition, poetic logic is used throughout the book, which is focused on relaying subjective experiences through language.
Are you transgender? Are you autistic (or ADHD)? This book is a tiny piece of our shared history. I’m sharing my story in hopes that we cannot be erased.
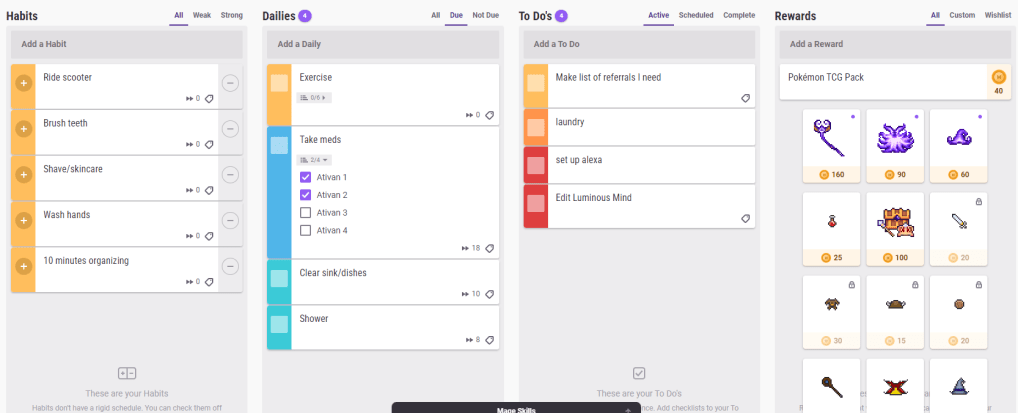
It seems like everyone’s got their own favorite app for managing daily tasks and to-dos, but so far my favorite is Habitica. I think it could be really useful for neurodivergent people with the right personality — Habitica is very much a “menus” game. If you love fine-tuning and deep personalization, Habitica could be perfect for you.
Habitica is available as both an app and a web interface. They both have utility, which I’ll discuss, and having both available may be great if you spend a lot of time at your desk. It is free with paid upgrades available; I haven’t paid for any upgrades and none of the features I’ll mention in my review are paid features. When you start playing (we are “playing” since Habitica is all about gamification, or turning your life’s to-do list into a game) you get a pixel avatar, which you can level up, equip items and pets to, and more. But the pixel avatar isn’t even the best feature of Habitica, in my opinion. You could play quite efficiently paying no attention to the avatar at all — more on this later.
It’s possible to use two or even three different apps to track all of these kinds of tasks. A more precise definition:
Habits: Tasks you want to do regularly (or reduce doing — habits can be negative), but that don’t have a fixed schedule for their occurrence.
Dailies: Tasks you want to do at specific times, for example, every day, or every 3 days, or every Tuesday and Thursday.
To-dos: Tasks you need to do once.
Each task can have checklist items, which increase the value of the task. In fact, there’s a pretty crazy level of detail and precision that can be attained in the settings menu for each task. And the system can have a learning curve, but that in itself makes the system appealing for menus-type people.
For neurodivergent people, it’s important any app can be flexible to avoid overwhelming us. Habitica normally inflicts damage on your character for missing dailies — however, there is an option in the setting menu to pause damage. No damage will be inflicted on you until you turn damage back on again and there is no cost or downside to pausing damage. You can continue to get rewards as usual.
Habitica comes with many built-in rewards, including items for your avatar, eggs and hatching potions (which create pets), and so on. But the primary currency of the game is gold, and you’re able to set custom rewards for in-game gold. I set up a Pokemon TCG pack for 40 gold. Any reward can be integrated into Habitica! Try using a preferred treat, video game time (or any favored activity), or small amounts of spending money as rewards.
The Habitica app allows you to choose from an impressive number of color themes, sound themes, and even custom app icons. Meanwhile, the web interface allows you to see everything you have to do at once — and gives the option to toggle tasks that are not due today so that they are invisible.
The thoughtful design and customization features of Habitica are what make it the best app I’ve used. It can be overwhelming, though, for people intimidated by those features. But it’s free, so why not give it a try?
*I am not affiliated with Habitica.

My name is Elliot. I’m an autistic psychologist with bipolar 1 disorder (and ADHD). I’ve been mentioned in passing [1] [2] in news articles about autistic autism researchers, but I prefer to keep on the science side of things. I usually only use Twitter for personal entertainment, sometimes biting my tongue as I weigh the pros and cons of engaging in autism discourse. I don’t entangle myself too deeply in advocacy work. For the most part, I keep my opinions on controversial things low-key no matter which side I am on. This post is a divergence from that tendency.
I have not uncommonly heard people object to classifying autism as a mental illness. It’s almost taken for granted that autism doesn’t fall under that umbrella. You may be surprised to know how people try to justify it if you actually ask them “Why isn’t it a mental illness?” Indeed, when pressed the most common responses are along the lines of:
The common element in all of these responses is a lack of understanding of what mental illness is and what mentally ill people experience. The question I want to ask back is this: If autism isn’t a mental illness, what is?
I’m not unsympathetic to the cause of not labeling people as having an “illness” because they’re neurodivergent, but why is it okay to do it to schizophrenic folks and not to autistic folks? There are plenty of mad people who don’t exactly view their diagnosis as an illness, although opinions in the psychiatric community are varied on this topic. Some consider diagnostic labels to be a prison, and others a gift. We sure live with plenty of labels.

Mental illness takes many forms. Some of them are quite properly classified as “neurodevelopmental disabilities” (including schizo spec, bipolar disorder, and ADHD — among possibly many others). The disorders I just mentioned are predominantly caused by genetics, and are therefore present at birth. The expression does change over time — but don’t autistic people have qualities that change as they grow and learn?
People refuse to acknowledge the close similarities between autism and schizophrenia (and other severe mental illness).
I’m going to flat-out recognize this: I think a lot of our community is biased. There are a lot of autistic people that are sanist, and they’ve been permitted to perpetuate misunderstanding.
My own therapist once tried to convince me after I admitted to experiencing delusions earlier in the week that I was merely referencing thoughts that were “overly rigid” as a result of my autism. My psychotic symptoms were being falsely attributed to my autism, and a lack of care was being given where care was needed.
And in the real world autistic people are at high risk of being mistaken for schizophrenic and taken to an ER for psych evaluation when they’re in distress. People can be treated horribly. But instead of stepping back and saying “Why do we treat mentally ill people horribly?” we’ve decided that allyship is not for us and we double down on “Autism isn’t a mental illness.” We cast non-autistic (and some autistic!) neurodivergent people as the Other.
To be quite honest, I think some autistic people are scared of crazy.
Perhaps they’re scared of people who may be erratic, hard to predict, or have dramatic emotional reactions.
Are there reasons to set autism apart from conditions we consider “mental illness”? I just don’t see the justification for viewing autism as so singularly unique from other conditions. It’s possible that, in the future, we could redefine and do away with the label of “mental illness” altogether. I’ll be interested to see how language evolves for neurodivergent folks. I hope even moreso that people in the autistic community approach the psychiatric community with an open mind, and not with fear or prejudice. I see hope for a future of cross-disability solidarity.

About two weeks ago, my cousin’s husband died from SUDEP (Sudden Unexpected Death in Epilepsy). He showed no signs of having experienced a seizure (no biting his tongue, for example); he simply went to bed one night and never woke up. He is bereaved by his daughter, who turned 7 years old a few days ago, and my cousin.
My cousin turned to me to talk about SUDEP. I warned her that while I knew this would be a difficult topic to discuss, I had a tendency to be very blunt about these things. But it turns out that’s exactly what she was looking for. She wanted to know the truth: Was there anything she could have done differently? And almost everyone on the planet would have told her no, because it’s the “right” answer. But she wasn’t looking for the “right” answer. She was looking for the “true” answer.
I explained that SUDEP doesn’t always follow a major seizure (it’s different than dying from status epilepticus). If the brain is like a computer, then a seizure is like a glitch, and SUDEP is like a system failure. Sometimes your screen glitches up and recovers. Sometimes it glitches and shuts down. But sometimes a broken computer just shuts down with no warning at all. In the latter case, there is nothing that could be done.
Neurodivergent people are often told that we need to be softer in our social approach — less honest, direct, blunt, or whatever you want to call it. But I’m a big believer in playing to our strengths. People with autism, ADHD, bipolar disorder, and other conditions have unique ways of communicating that have value. My cousin later told me that she understood my computer metaphor and it helped her, just a little bit, to begin the process of moving on with the rest of her life.
There’s nothing wrong with being a “blunt” communicator. Sometimes, that’s exactly what is needed. There are a lot of autistic people who won’t lie to you just to make you feel better, and that in itself is actually a virtue.
As for bipolar disorder, I think a lot of us have highly emotional communication styles. There are always going to be situations where this comes in handy, even if some people consider it a downside. People have always been open with me about their suicidal ideation or urges to self-harm because they knew I could take it and I would be there for them without freaking out or telling them they needed to go to the hospital if they didn’t really.
All neurodiverse people have their own styles of communicating, and they all come with benefits in the right situation. What do you think?

A lot of people with conditions that are defined in the DSM (Diagnostic and Statistical Manual of Mental Disorders) disagree with what their condition is called. In this post, I’m going to muse over changing the names of psychiatric disorders.
When the DSM-III was published, the DSM committee decided that the term “manic depression” had become overly stigmatized and abused. There was little to no change in the diagnostic features or description of the disorder (which has actually been fairly consistent for a very long time!), the only reason for changing the terminology was political. Many years later, I feel this has resulted in the term “bipolar” being just as stigmatized as “manic depression” ever was — except it’s even more abusable, since “bipolar” can be used as an adjective to describe many things, famously including the weather.
It should’ve been obvious that the stigma of manic depression didn’t originate from the term “manic depression” — and therefore not shocking that the same stigma followed, not the term that was used, but the people who live with the disorder. It was always the people, never the term. On top of that, I feel “manic depression” is more accurate as the term “bipolar disorder” doesn’t portray the common reality of mixed episodes and mixed mood presentation. “Bipolar” seems to imply a state of bistability, where two states representing opposite ends of one dimension (mania and depression) are cleanly and abruptly switched between; bipolar can be like this, but it is often messier.
ADHD is a controversial term for some advocates and it’s understandable why. While attention and hyperactivity/impulsivity are characteristics that are used to diagnose the disorder, they’re downstream of the real difference experienced by people who live with the condition — which is developmental effects on executive functioning. Broadening the term to define it by its root cause would probably feel more accurate of the experience of living with the condition.
Inadvertently, if the diagnostic criteria were changed accordingly to reflect other developmental disorders of executive dysfunction, there may be groups of people who didn’t meet the criteria before who now do. This is something to be interested in, of course. Attention and hyperactivity/impulsivity could still be used as specifiers, and the developmental history aspects would probably still be required so that people with executive dysfunction of non-developmental origin aren’t accidentally included. Additionally, we know that autism is associated with some kinds of executive dysfunction and this change would probably blur the lines between them even more — but in reality, those lines are pretty blurry.
There is a lot of controversy over this one, and to be honest I don’t have all of the answers. I think “Asperger’s” was a term of limited utility because many studies could not find clear differences between “Asperger’s” and “High Functioning Autism” even though supposedly the Asperger’s group had no language delay and the HFA group did. Their outcomes, though, were the same. So it was decided that we would collapse autism into one diagnosis that represents a gradient or spectrum of features and levels of impact on the person’s life.
However, I actually agree with some advocates who say that this has proven obtrusive for people with high support needs as the common conception of autism drifts further and further from Rain Main to Sheldon Cooper. There are many people out there who no longer believe autism is a disability. I can’t fully reconcile myself with this stance when we’re talking about a nonverbal adult with an IQ of 40: this person’s life is much, much different than mine, and I genuinely want to help them in the most effective way I can. At this venture, I believe we need a term for people with high support needs. But, the options thus far have been problematic (for example, I do see the reasons why “high functioning” and “low functioning” are much too simplistic to capture meaningful differences).
In the end, the best I can come up with right now is to include Verbal IQ score as a specifier. It’s not perfect (we know IQ means something specific, and can’t be generalized to “intelligence”), but it’s one of the better indicators we reliably have of how disabled this person is, how many barriers they’re going to face to get treated fairly and with respect. And, it doesn’t create a competition where someone is more or less autistic than I am. We’re both autistic; it’s just that one of us has an IQ of 40 and that information isn’t trite. Despite the risks of increasing discrimination, I think we’ve seen with the bipolar fiasco that changing terms merely to avoid stigma (which is attached to people, not to terms) is not a good idea.

Recently, on Twitter, I confessed that I had not been able to complete reading NeuroTribes (a very interesting book, and also a lengthy one). The other person insisted that a PhD student should be able to read a book and accused me of lacking academic integrity — basically, that I am lazy and don’t deserve my PhD.
I’m here to say that attitude is inherently ableist. But to give the benefit of the doubt, perhaps most people don’t know that bipolar disorder actually can affect your ability to read. I learned to read early as a child — I was a prolific consumer of text, and I had a college reading level in elementary school (this is called hyperlexia). But after being medicated for bipolar disorder, my ability to sustain focus and momentum while reading a long document has been very limited.
Lithium is probably the biggest offender. It kind of affects how you see words on the page — like a pseudo-dyslexia, the words seem kind of blurry and distorted. It can be impossible to read full books. I can still read journal articles because they generally have a defined structure and an abstract. I can also read poetry, which I enjoy. I recommend seeking out these kinds of texts if reading is something you struggle with.
Most of all, I want you to know that this is common, you are not alone in having an acquired inability to read and you still deserve your career, whatever that may be. It’s not a matter of “intellectual thoroughness”; it’s part of a disability, and it’s more common than you think.

I also find it difficult to watch videos, TV, or movies. The information conveyed through video media covers many modalities — sound (music), speech, visuals, movement (spatial), and the overall plot you’re supposed to be following. Sitting for the length of a movie is hard, but it’s also just hard to follow so many things at once. My brain gets overwhelmed with too much information of different kinds to process (evidence of poor sensory integration, a symptom of autism). But it helps to reduce the overload by using captions (combining speech with visuals, thus reducing the number of information modalities) or watching something animated, which compresses the demands of visual and spatial information greatly.

Have you ever had trouble consuming media?
What strategies have you used?

Whatever you want to call them — stims, repetitive behaviors, stereotypies — the terms are more-or-less interchangeable, but it remains that they are of importance in how we think about autism. The repetitive behavior/restricted interests domain is essential to an autism diagnosis. Autistic people, when asked, mostly seem to believe this is an important part of autism. Strangely, very few people have undertaken empirical research to validate (or challenge) common ideas about the nature of stimming.
For those who don’t know: what is stimming? There’s actually some variation in what people consider stims, but I think most people would agree that it includes rhythmic, repetitive movements of the body such as rocking, hand flapping, and pacing. Many people include vocalizations such as grunting or whistling. Based on the conventional description of some autistic children having a fascination with parts of objects (like the wheels on a toy car), I feel manipulation of items such as fidget toys and spinners should be counted as well.

Of course, then we’re get into restricted interests territory. Restricted interests and repetitive behaviors are counted in the same “domain” in the DSM, along with sensory atypicalities. In my view, they blend into each other, forming a continuum — but more on that later.
If you asked me, I’d say there’s a lot we don’t know about this topic. A lot of people have beliefs, for sure, but there’s little to no real evidence. At least, not the kind of evidence you can cite.
Most of the knowledge that’s out there comes from the beliefs of autistic community members. Dr. Steven Kapp (who is, coincidentally, a friend) did a qualitative analysis of 31 autistic people’s opinions on stimming.1 Nobody said they disliked their stimming; most people said they found it calming. The study thusly found that stimming most likely serves a regulatory function, and identified three factors that autistic people said caused their stimming behavior: overwhelming environment/sensory overload, noisy thoughts, and uncontainable emotion.
It’s interesting to me that nobody in this study mentioned under-stimulation of sensory input.1 They seemed more to believe that stimulation in excess of a certain individual or situational threshold was the primary cause, and in this case the “stimulation” could be an internal stimuli (a thought or an emotion).
It’s such a simple theory that it seems baffling that nobody has really tested it. Why is that important? Well… sometimes, as humans, things aren’t what we expect them to be. I know a lot of people will react negatively to that sentiment, but I’m autistic too, so it really is an everyone thing. A lot of psychology (ex, cognitive psychology) is actually not self-evident, and may be counter-intuitive. For example, people are not particularly good at judging how they best learn. People overestimate the benefit of massed rehearsal (cramming for an exam) because they feel like it helps them remember more than spaced rehearsal (studying every night), even after seeing evidence that spaced rehearsal results in better task performance.2
Don’t get me wrong, metacognitive insight is valuable — it’s my own greatest weapon! — but it helps to have evidence to back it up. (Likewise, it helps to have qualitative information to back up empirical results.) So why don’t we have studies about this?

One study that has been done (although, again, not an empirical study) used Bayesian statistical principles to think about the mechanisms of cognition in autism.3 They concluded that autism features atypical accuracy of predictions — or, more precisely, that they did not use as much prior knowledge in their perception, leading to potentially more accurate perceptions of the world. However, this makes ambiguity and uncertainty very difficult to deal with. The authors use this framework to understand stimming as a means of reducing the uncertainty in the environment, and thereby reducing the sense of alarm or sensory overload experienced by that person.
As I mentioned, repetitive behaviors blend together with restricted interests. Something I’ve become interested in is the role of perseverative or repetitive thoughts and its relation to the role of repetitive behaviors. I explored this idea a little bit in my first paper,4 but I have yet to truly investigate my thoughts on the matter as much as I would like. Here’s my underlying theory: autistic children, as children, have both repetitive behaviors and repetitive thoughts. Normally, these two processes inhibit each other. This seems to corroborate well with the accounts of “noisy thoughts” being a precursor for stimming behaviors to control them.1 However, when children with normative verbal ability become older, they stop doing repetitive behaviors — leading to increased repetitive thoughts, which my study found could be a risk factor for developing depression.4 This might explain, at least in part, why rates of depression are highest in autistic adults with more normative verbal ability. And it lines up quite well with what the autistic people in Kapp’s study said: they identified others’ tolerance of their stims as a matter of acceptance vs. devaluation.1
Do you have any theories?
There’s no doubt in my mind that Van Gogh had bipolar disorder. He had many symptoms related to bipolar disorder: manic episodes, depressive episodes, hallucinations, sleep disturbance, substance abuse, memory problems, nightmares, and anxiety, to name a few from his asylum files.
Yet, additional diagnostic labels could help to clarify his overall presentation. One diagnosis that has been put forward is BPD. It does seem to explain some of the events of his life, for example, his heated interpersonal conflicts and fears of abandonment related to Paul Gauguin. However, a diagnosis of autism has not been seriously considered. This is interesting in light of the heightened prevalence of bipolar disorder in autism — an autistic person is as much as 8.5 times more likely to have bipolar disorder than a non-autistic person (this number assumes no intellectual disability and a diagnosis before age 28).1 Another study found that 7% of autistic people also had bipolar disorder.2

As a child Van Gogh was described by his younger sister as “intensely serious and uncommunicative, and walked around clumsily as if in a daze, with his head hung low”, and went on to say that he was like a stranger both to his siblings and to himself. A servant said he was “an odd, aloof child who had queer manners and seemed more like an old man” than a child.3 These are characteristics often ascribed to some autistic children, even poor motor coordination (dyspraxia).
Vincent was deeply intelligent, thoughtful, and demonstrated what seemed like the capacity to be successful, but as a young man he struggled to find a vocation that could accommodate him. He drifted from an art dealership (where he was fired for arguing with buyers), to a teaching job, to a minister’s assistant for a Methodist church, to a bookshop where he reportedly doodled and translated parts of the Bible into English, French, and German, to religious studies. He failed his entrance exam in theology and his missionary course. Religion was a special interest for Van Gogh. He was endlessly devoted and passionate about the subject, but his odd behavior made him an ineffective preacher, and he was not a good student.

Van Gogh had severe social problems which seem to have started early in his life. People repeatedly thought that he was odd, and they didn’t want to be around him. His peculiarities were off-putting. Children were scared of him. Scholars suggest that he did not understand the concepts of diplomacy or salesmanship, that he lacked insight into the thought processes of others, and lacked the ability to cognitively understand their emotions and motivations.3 He was emotionally dysregulated and prone to agitated or impulsive meltdown behaviors. As his interest in painting became more intense and all-consuming, he neglected maintenance of his body or appearance, appearing even more eccentric.
One of the highlights of Van Gogh’s medical files that has yet to be parsimoniously explained is his chronic stomach issues. In particular, gastrointestinal problems seem to be an important feature of autism4 although bipolar disorder may also be related to stomach problems.

Finally, there’s the most obvious trait of Van Gogh’s: his artistic ability. Many people have suggested that Vincent might have had some form of synesthesia. Further, I hypothesize that hue discrimination may, like pitch discrimination, be enhanced in some autistic people.5
A diagnosis of autism didn’t exist in Van Gogh’s time — in fact, wouldn’t exist for over 50 years after his death. Perhaps it’s not so surprising that the autism connection has been overlooked. Vincent van Gogh’s wild, reckless nature combined with intellectual and artistic sensibilities (and lack of mathematical talent) defies narrow stereotypes of autism, yet embodies a certain reality of it: he was thoughtful yet lacked insight, seen as a stranger by the world around him while experiencing the world as fundamentally strange, and possessed incredible gifts yet was understood as deficient. Maybe it’s time to look beyond famous scientists and mathematicians for autistic historical figures.
1. Selten J-P, Lundberg M, Rai D, Magnusson C. Risks for nonaffective psychotic disorder and bipolar disorder in young people with autism spectrum disorder: A population-based study. JAMA Psychiatry. 2015;72(5):483-489. doi:10.1001/jamapsychiatry.2014.3059
2. Skokauskas N, Frodl T. Overlap between autism spectrum disorder and bipolar affective disorder. Psychopathology. 2015;48(4):209-216. doi:10.1159/000435787
3. Butterfield, B. The Troubled Life of Vincent Van Gogh. Vincent van Gogh website. September 21, 2002. Accessed May 24, 2020.
http://www.geocities.com/Paris/Louvre/9633/VincentVanGogh.htm
4. Adams JB, Johansen LJ, Powell LD, Quig D, Rubin RA. Gastrointestinal flora and gastrointestinal status in children with autism – comparisons to typical children and correlation with autism severity. BMC Gastroenterol. 2011;11. doi:10.1186/1471-230X-11-22
5. Heaton P, Williams K, Cummins O, Happé F. Autism and pitch processing splinter skills: A group and subgroup analysis. Autism. 2008;12(2):203-219. doi:10.1177/1362361307085270
