A little while back, I started looking around to make a kit of stim tools that I could use to help me sit through long meetings and lectures. Although the combination I’ve settled on (for now) isn’t perfect, I thought it might be helpful to share what I’ve learned and what I’m doing right now.
Why use stim tools?
It’s widely known that autistic people make use of stim tools like the ones I’m going to be talking about. For autistic people, using stim tools may be a method of stimming or “repetitive behaviors”. Many ADHDers use stim tools as well. However, it’s not just autistics and ADHDers who can benefit; for example, bipolar people can definitely use them, particularly in a manic (or mixed) phase. Stim tools can also be used by people who struggle with compulsive behaviors like skin picking (dermatillomania) or hair pulling (trichotillomania). Finally, stim tools can be used to help anyone, regardless of diagnosis!
Making a stim kit
I started out making a single stim kit, but I soon found it might be more beneficial to make several kits of different sizes. However, the first “stim kit” I want to talk about doesn’t usually come out of a box or a bag — I’m talking about wearable stim tools! Chewable necklaces are very popular among people who bite their nails or non-chewable objects such as pencils. Mine, though, is a little different…
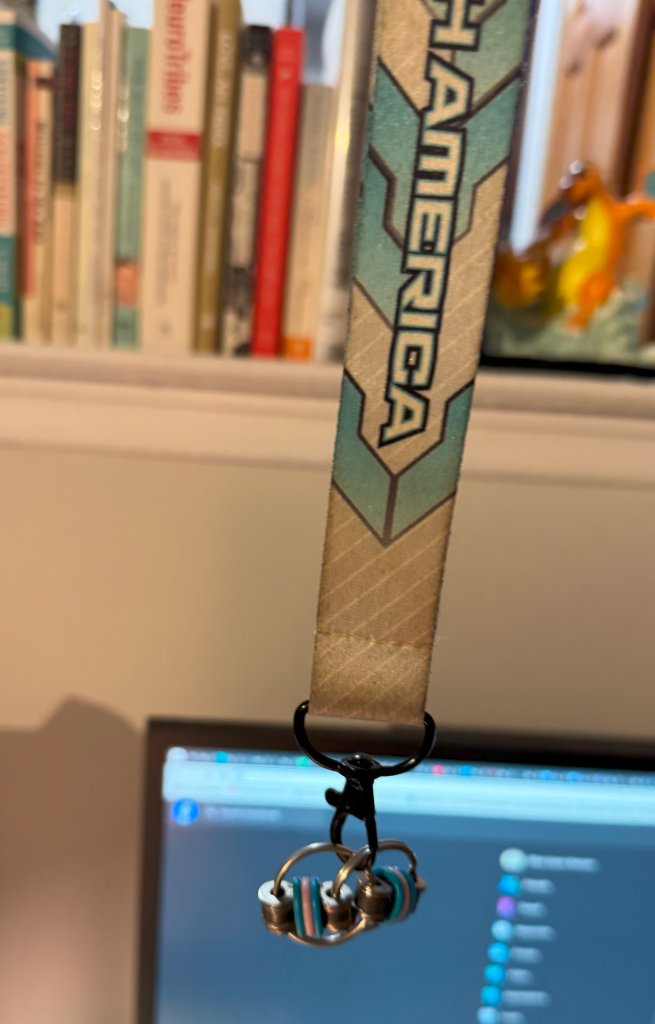
I made this out of a lanyard (this one is from the Pokémon North American International Championships a few years ago) and a bike chain keyring fidget. This is often my go-to stim tool as I wear it around my neck and don’t have to fumble around in my bag for it. It’s also pretty cheap; there are multiple Etsy listings for $5 plus shipping (like this one) and even listings for fun pride-themed colorways which I might just buy right now! Be right back! (By the way, I have no affiliation with any of the products I may link to in this article, nor am I receiving any compensation for including them.) Anyway, these little fidgets are silent, small, and I think they make a particularly satisfying stim for people who may be prone to skin picking. And you can use any lanyard your heart desires!
Now, onto the actual stim kits…
Pocket kit

I’ll call the smallest one the “pocket kit” because it just fits in the front pockets of my jeans (American Eagle Womens’ Jeggings). It easily fits in the front pocket of my mini backpack, as well as my bigger backpacks. As you can see, I’m using a Pokémon box (this will be a theme) which is on sale at the Pokémon Center for $20. It also comes with dice and cute status markers for playing Pokémon Trading Card Game, but my favorite asset was this box. So what’s in it?

- Magnetic Haptic Slider from clickbricks — I like this stim tool a lot! It’s not completely silent, but it’s quiet enough to fly under the radar in most situations. To me it feels kind of like flicking a lighter, which is something I do… a lot.
- Another keyring bike chain fidget!
- Nicotine gum, for reasons stated above…
- One stick of Crystal Light lemonade and one bag of Tazo Earl Grey tea.
I’m looking for new stim tools that will fit in the pocket kit, so if you have any recommendations, please send them to me! I really want to hear from you.
Next, the medium kit…
Medium Kit

This one is also related to Pokémon! It’s a Japanese deck box. One of my favorites, so it seems fitting I put some stim tools in there. If you’re not familiar with deck boxes, they are generally not too large. I think this one is around 3 in (height) x 3 in (depth) x 4 in (width). The NeeDoh Nice Cube just fits inside.

- NeeDoh Nice Cube — I love this squishable sensory tool! It’s a little bit like a stress ball but it feels soft/gooey, almost like putty or slime. It’s not as sticky, though. It’s got a nice weight to it and the size is perfect for my hands. That said, they make other products at NeeDoh; the cube is probably the most popular.
- Infinity Cube — I got this one at a gas station somewhere on Long Island, but the Etsy creator who I linked carries some really cool colors and right now they’re on sale for $3. Totally worth it! Infinity cubes can be folded into different configurations almost, well, infinitely. I’ve enjoyed using this one for years now. It’s a tried and true inclusion.
- Fidget Cube — The fidget cube isn’t my favorite fidget, but I do like some of its functionalities. It is nearly silent. I like the buttons (especially the clicky ones, which do make a subdued sound) as well as the switch/lever and the thumbpad (circular appendage).
That’s right… everything in the medium kit is a cube! (✿◡‿◡) A happy little accident.
Large kit

Now, I don’t want to lie to you, so here it is: a fidget spinner can just barely fit in the deck box I’m using for the medium kit. But, I’m afraid of doing damage to the box by overloading it… so my 2 fidget spinners were included in this amazing bag I got from the Pokémon Center. It’s sparkly! But any toiletry bag should do. Pick your favorite or buy one that suits you!

- 2 fidget spinners — The blue sparkly one is plastic and lighter than the iridescent metal one. They were both gifts and I quite enjoy using them during long lectures.
- Another bike chain keyring fidget in “unicorn” colors.
- Tangle Therapy Relax — Has textured segments with a slightly give to them. I generally like to manipulate it in my hand and don’t like pulling the pieces apart, but Tangles are good for either!
- Keyboard fidget — This uses mechanical keyboard testers as a stim tool! Mine is 4×1 keys and uses Blue switches (Cherry MX I believe?), so it’s quite clicky and noisy, like typing on a typewriter. However, this listing on etsy says they also have linear switches (which are much quieter) and I bet they could even use both!
Have I missed an important stim? Let me know in the comments!
Atmosphere stims
There are some stim tools that can’t be carried around in a box or a bag, but rather, are meant to be used at home or in a private space. Here are some of those things:
- Candles/incense/air freshener — I highly recommend Morning Star incense!! They even come with a little holder.
- Weighted blanket or sleep pod
- Bubble bath or epsom salts
- Large stuffies — I have a Pikachu!
- Swings, indoor or outdoor
- A medium-sized fan — or bigger; for summer
So that’s what I’ve learned! Share in the comments your favorite stim tools and how they help you!