













A little while back, I started looking around to make a kit of stim tools that I could use to help me sit through long meetings and lectures. Although the combination I’ve settled on (for now) isn’t perfect, I thought it might be helpful to share what I’ve learned and what I’m doing right now.
It’s widely known that autistic people make use of stim tools like the ones I’m going to be talking about. For autistic people, using stim tools may be a method of stimming or “repetitive behaviors”. Many ADHDers use stim tools as well. However, it’s not just autistics and ADHDers who can benefit; for example, bipolar people can definitely use them, particularly in a manic (or mixed) phase. Stim tools can also be used by people who struggle with compulsive behaviors like skin picking (dermatillomania) or hair pulling (trichotillomania). Finally, stim tools can be used to help anyone, regardless of diagnosis!
I started out making a single stim kit, but I soon found it might be more beneficial to make several kits of different sizes. However, the first “stim kit” I want to talk about doesn’t usually come out of a box or a bag — I’m talking about wearable stim tools! Chewable necklaces are very popular among people who bite their nails or non-chewable objects such as pencils. Mine, though, is a little different…
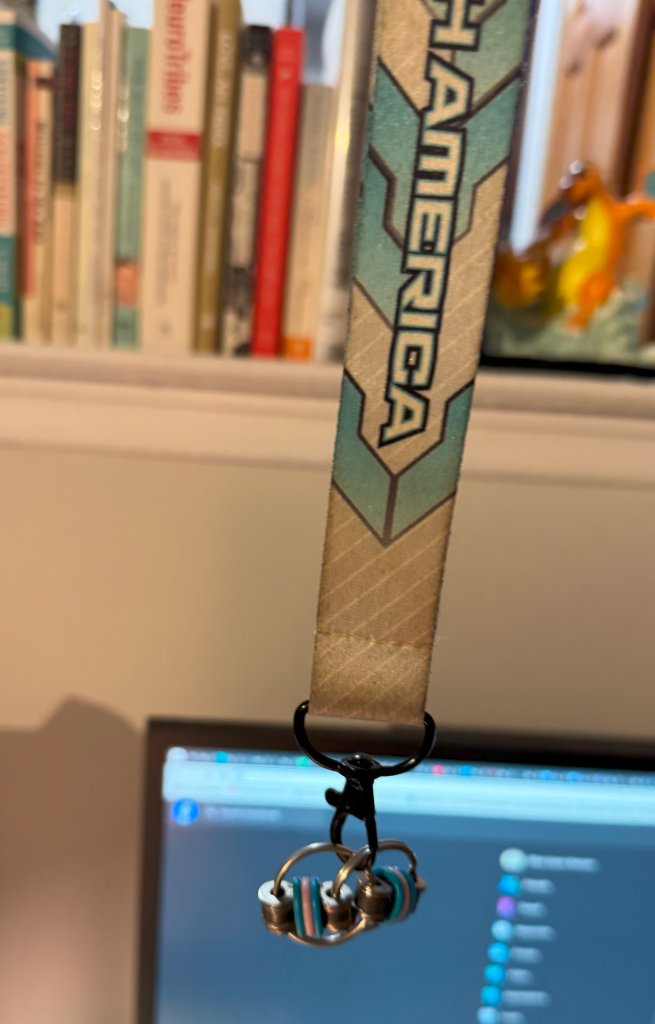
I made this out of a lanyard (this one is from the Pokémon North American International Championships a few years ago) and a bike chain keyring fidget. This is often my go-to stim tool as I wear it around my neck and don’t have to fumble around in my bag for it. It’s also pretty cheap; there are multiple Etsy listings for $5 plus shipping (like this one) and even listings for fun pride-themed colorways which I might just buy right now! Be right back! (By the way, I have no affiliation with any of the products I may link to in this article, nor am I receiving any compensation for including them.) Anyway, these little fidgets are silent, small, and I think they make a particularly satisfying stim for people who may be prone to skin picking. And you can use any lanyard your heart desires!
Now, onto the actual stim kits…

I’ll call the smallest one the “pocket kit” because it just fits in the front pockets of my jeans (American Eagle Womens’ Jeggings). It easily fits in the front pocket of my mini backpack, as well as my bigger backpacks. As you can see, I’m using a Pokémon box (this will be a theme) which is on sale at the Pokémon Center for $20. It also comes with dice and cute status markers for playing Pokémon Trading Card Game, but my favorite asset was this box. So what’s in it?

I’m looking for new stim tools that will fit in the pocket kit, so if you have any recommendations, please send them to me! I really want to hear from you.
Next, the medium kit…

This one is also related to Pokémon! It’s a Japanese deck box. One of my favorites, so it seems fitting I put some stim tools in there. If you’re not familiar with deck boxes, they are generally not too large. I think this one is around 3 in (height) x 3 in (depth) x 4 in (width). The NeeDoh Nice Cube just fits inside.

That’s right… everything in the medium kit is a cube! (✿◡‿◡) A happy little accident.

Now, I don’t want to lie to you, so here it is: a fidget spinner can just barely fit in the deck box I’m using for the medium kit. But, I’m afraid of doing damage to the box by overloading it… so my 2 fidget spinners were included in this amazing bag I got from the Pokémon Center. It’s sparkly! But any toiletry bag should do. Pick your favorite or buy one that suits you!

Have I missed an important stim? Let me know in the comments!
There are some stim tools that can’t be carried around in a box or a bag, but rather, are meant to be used at home or in a private space. Here are some of those things:
So that’s what I’ve learned! Share in the comments your favorite stim tools and how they help you!
It seems like everyone’s got their own favorite app for managing daily tasks and to-dos, but so far my favorite is Habitica. I think it could be really useful for neurodivergent people with the right personality — Habitica is very much a “menus” game. If you love fine-tuning and deep personalization, Habitica could be perfect for you.
Habitica is available as both an app and a web interface. They both have utility, which I’ll discuss, and having both available may be great if you spend a lot of time at your desk. It is free with paid upgrades available; I haven’t paid for any upgrades and none of the features I’ll mention in my review are paid features. When you start playing (we are “playing” since Habitica is all about gamification, or turning your life’s to-do list into a game) you get a pixel avatar, which you can level up, equip items and pets to, and more. But the pixel avatar isn’t even the best feature of Habitica, in my opinion. You could play quite efficiently paying no attention to the avatar at all — more on this later.
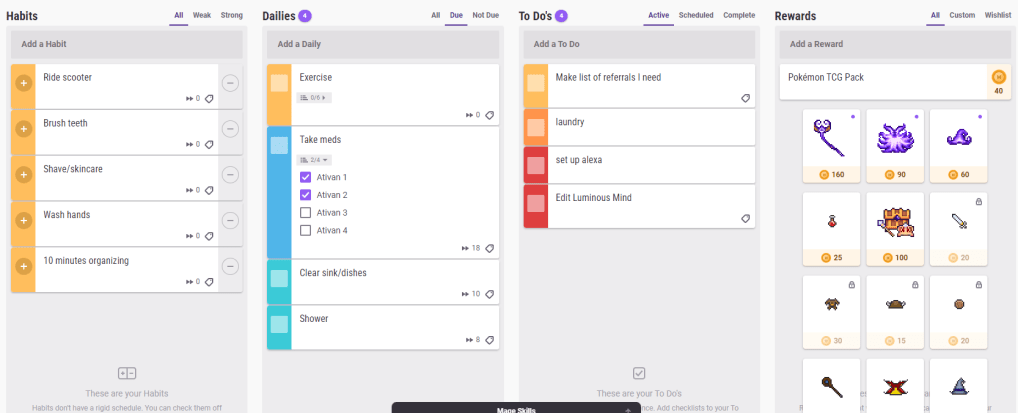
It’s possible to use two or even three different apps to track all of these kinds of tasks. A more precise definition:
Habits: Tasks you want to do regularly (or reduce doing — habits can be negative), but that don’t have a fixed schedule for their occurrence.
Dailies: Tasks you want to do at specific times, for example, every day, or every 3 days, or every Tuesday and Thursday.
To-dos: Tasks you need to do once.
Each task can have checklist items, which increase the value of the task. In fact, there’s a pretty crazy level of detail and precision that can be attained in the settings menu for each task. And the system can have a learning curve, but that in itself makes the system appealing for menus-type people.
For neurodivergent people, it’s important any app can be flexible to avoid overwhelming us. Habitica normally inflicts damage on your character for missing dailies — however, there is an option in the setting menu to pause damage. No damage will be inflicted on you until you turn damage back on again and there is no cost or downside to pausing damage. You can continue to get rewards as usual.
Habitica comes with many built-in rewards, including items for your avatar, eggs and hatching potions (which create pets), and so on. But the primary currency of the game is gold, and you’re able to set custom rewards for in-game gold. I set up a Pokemon TCG pack for 40 gold. Any reward can be integrated into Habitica! Try using a preferred treat, video game time (or any favored activity), or small amounts of spending money as rewards.
The Habitica app allows you to choose from an impressive number of color themes, sound themes, and even custom app icons. Meanwhile, the web interface allows you to see everything you have to do at once — and gives the option to toggle tasks that are not due today so that they are invisible.
The thoughtful design and customization features of Habitica are what make it the best app I’ve used. It can be overwhelming, though, for people intimidated by those features. But it’s free, so why not give it a try?
*I am not affiliated with Habitica.

About two weeks ago, my cousin’s husband died from SUDEP (Sudden Unexpected Death in Epilepsy). He showed no signs of having experienced a seizure (no biting his tongue, for example); he simply went to bed one night and never woke up. He is bereaved by his daughter, who turned 7 years old a few days ago, and my cousin.
My cousin turned to me to talk about SUDEP. I warned her that while I knew this would be a difficult topic to discuss, I had a tendency to be very blunt about these things. But it turns out that’s exactly what she was looking for. She wanted to know the truth: Was there anything she could have done differently? And almost everyone on the planet would have told her no, because it’s the “right” answer. But she wasn’t looking for the “right” answer. She was looking for the “true” answer.
I explained that SUDEP doesn’t always follow a major seizure (it’s different than dying from status epilepticus). If the brain is like a computer, then a seizure is like a glitch, and SUDEP is like a system failure. Sometimes your screen glitches up and recovers. Sometimes it glitches and shuts down. But sometimes a broken computer just shuts down with no warning at all. In the latter case, there is nothing that could be done.
Neurodivergent people are often told that we need to be softer in our social approach — less honest, direct, blunt, or whatever you want to call it. But I’m a big believer in playing to our strengths. People with autism, ADHD, bipolar disorder, and other conditions have unique ways of communicating that have value. My cousin later told me that she understood my computer metaphor and it helped her, just a little bit, to begin the process of moving on with the rest of her life.
There’s nothing wrong with being a “blunt” communicator. Sometimes, that’s exactly what is needed. There are a lot of autistic people who won’t lie to you just to make you feel better, and that in itself is actually a virtue.
As for bipolar disorder, I think a lot of us have highly emotional communication styles. There are always going to be situations where this comes in handy, even if some people consider it a downside. People have always been open with me about their suicidal ideation or urges to self-harm because they knew I could take it and I would be there for them without freaking out or telling them they needed to go to the hospital if they didn’t really.
All neurodiverse people have their own styles of communicating, and they all come with benefits in the right situation. What do you think?

A lot of people with conditions that are defined in the DSM (Diagnostic and Statistical Manual of Mental Disorders) disagree with what their condition is called. In this post, I’m going to muse over changing the names of psychiatric disorders.
When the DSM-III was published, the DSM committee decided that the term “manic depression” had become overly stigmatized and abused. There was little to no change in the diagnostic features or description of the disorder (which has actually been fairly consistent for a very long time!), the only reason for changing the terminology was political. Many years later, I feel this has resulted in the term “bipolar” being just as stigmatized as “manic depression” ever was — except it’s even more abusable, since “bipolar” can be used as an adjective to describe many things, famously including the weather.
It should’ve been obvious that the stigma of manic depression didn’t originate from the term “manic depression” — and therefore not shocking that the same stigma followed, not the term that was used, but the people who live with the disorder. It was always the people, never the term. On top of that, I feel “manic depression” is more accurate as the term “bipolar disorder” doesn’t portray the common reality of mixed episodes and mixed mood presentation. “Bipolar” seems to imply a state of bistability, where two states representing opposite ends of one dimension (mania and depression) are cleanly and abruptly switched between; bipolar can be like this, but it is often messier.
ADHD is a controversial term for some advocates and it’s understandable why. While attention and hyperactivity/impulsivity are characteristics that are used to diagnose the disorder, they’re downstream of the real difference experienced by people who live with the condition — which is developmental effects on executive functioning. Broadening the term to define it by its root cause would probably feel more accurate of the experience of living with the condition.
Inadvertently, if the diagnostic criteria were changed accordingly to reflect other developmental disorders of executive dysfunction, there may be groups of people who didn’t meet the criteria before who now do. This is something to be interested in, of course. Attention and hyperactivity/impulsivity could still be used as specifiers, and the developmental history aspects would probably still be required so that people with executive dysfunction of non-developmental origin aren’t accidentally included. Additionally, we know that autism is associated with some kinds of executive dysfunction and this change would probably blur the lines between them even more — but in reality, those lines are pretty blurry.
There is a lot of controversy over this one, and to be honest I don’t have all of the answers. I think “Asperger’s” was a term of limited utility because many studies could not find clear differences between “Asperger’s” and “High Functioning Autism” even though supposedly the Asperger’s group had no language delay and the HFA group did. Their outcomes, though, were the same. So it was decided that we would collapse autism into one diagnosis that represents a gradient or spectrum of features and levels of impact on the person’s life.
However, I actually agree with some advocates who say that this has proven obtrusive for people with high support needs as the common conception of autism drifts further and further from Rain Main to Sheldon Cooper. There are many people out there who no longer believe autism is a disability. I can’t fully reconcile myself with this stance when we’re talking about a nonverbal adult with an IQ of 40: this person’s life is much, much different than mine, and I genuinely want to help them in the most effective way I can. At this venture, I believe we need a term for people with high support needs. But, the options thus far have been problematic (for example, I do see the reasons why “high functioning” and “low functioning” are much too simplistic to capture meaningful differences).
In the end, the best I can come up with right now is to include Verbal IQ score as a specifier. It’s not perfect (we know IQ means something specific, and can’t be generalized to “intelligence”), but it’s one of the better indicators we reliably have of how disabled this person is, how many barriers they’re going to face to get treated fairly and with respect. And, it doesn’t create a competition where someone is more or less autistic than I am. We’re both autistic; it’s just that one of us has an IQ of 40 and that information isn’t trite. Despite the risks of increasing discrimination, I think we’ve seen with the bipolar fiasco that changing terms merely to avoid stigma (which is attached to people, not to terms) is not a good idea.

I had always thought I had ADHD inattentive type. However, when I recently asked my psychiatrist (out of curiosity) she chuckled and said that, in her clinical opinion, I have the combined type.
Part of my perception may come from that fact that, due to my mild cerebral palsy, I move at a much slower pace than other people — thereby masking some apparent “hyperactivity”. To complicate matters, I’m currently taking two antipsychotics (Thorazine/chlorpromazine and Zyprexa/olanzapine) both of which can cause side effects that are phenotypically similar to hyperactivity (this is called akathisia). But how much of that is the drug per se, and how much of it is my ADHD (which may, in turn, be worsened by the drug)?
I think there’s a broader misconception at play. We simply do not know how to identify hyperactivity in developmental adults.

First off, let’s get some facts straight. In adults with ADHD, it’s more common to have symptoms of inattention (about 90% have these kinds of symptoms in a prominent way) while only about half of adults display clinically relevant hyperactivity or impulsivity1. By implication, we can assume that the population of adults with ADHD breaks down something like this: 10% have hyperactive type, 40% have combined type, and 50% have inattentive type. Those numbers may be a little off, but it’s a good place to start.
Yet, even though it is acknowledged that adults have hyperactivity and impulsivity, these symptoms are not well understood in adults — at least, they aren’t characterized as well as they are for children. And the presentation of these symptoms changes over the lifespan. It is thought by researchers that hyperactivity decays as the ADHD child becomes an adult, while inattention persists1.
Here are diagnostic criteria for hyperactivity and impulsivity in ADHD1:
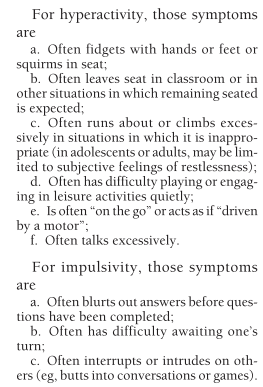
Without a doubt these symptoms intentionally mirror those used for children, with some addendums (instead of running and climbing excessively, we just think about doing it — leading to “subjective feelings of restlessness”). Somehow, some adults with ADHD have internalized our externalizing behaviors. Instead of running from wall to wall like a four-year-old, I just feel this incredible tension in my body created by Not Moving. But it’s all inside my head. You can’t see it unless you look very closely.
I can see myself in this list of symptoms, nonetheless. I fidget, I stim, I stand when I’m supposed to remain seated, I feel restless constantly, I interrupt others when they are speaking, I feel a kind of somatic pain or intense pressure and frustration when I have to wait a long time for something that’s right in front of me.
But there is an element here that we are not capturing.

We know from literature in children that hyperactivity/impulsivity and inattention are correlated. But, it’s not so clear what the relationship is, and it really gets at the core deficit we’re trying to get at with an ADHD diagnosis: poor executive functioning and self-regulation. I can’t focus my attention, so I pace around for hours, smoking cigarettes on the patio. I feel like I have to keep moving; I constantly have to be doing something, even if I’m doing nothing. I can’t relax. That isn’t good for a child, and it’s even less so for an adult. My body feels tense and worn, like a pair of old shoes.
It turns out, too, that ADHD in adults is associated with lower socio-economic status, lower levels of academic achievement, problems with relationships, and even poorer driving ability and more traffic violations1.
Not long ago children with ADHD were presupposed to exist in a liminal state: it was thought that ADHD was a disorder of childhood, and that it diminishes with developmental advancement. Yet research (including various brain anatomy, neuroimaging, and genetics studies) is showing that this is not the case1.
Ironically enough, it’s time to turn our attention to adults with ADHD. Although it does make some sense that classic symptoms of hyperactivity decline with age, I am interested in how hyperactivity later manifests in adults who no longer fit the typical, child-centered definition of hyperactivity.
Personally, I think inwardly-turned hyperactivity may be one of the driving forces behind high levels of depression and anxiety seen in adults with ADHD. Around half of adults with ADHD have had one or more major depressive episode, and around half of adults with ADHD have one or more clinical anxiety disorder2.
There’s also a fascinating overlap with bipolar disorder, which may be a blog post for another day!
Are you an adult with ADHD? Have you ever met criteria for hyperactive or combined type ADHD, either now or as a child? Share your experiences!
